By Susi Hately, B.Sc. Kin, C-IAYT 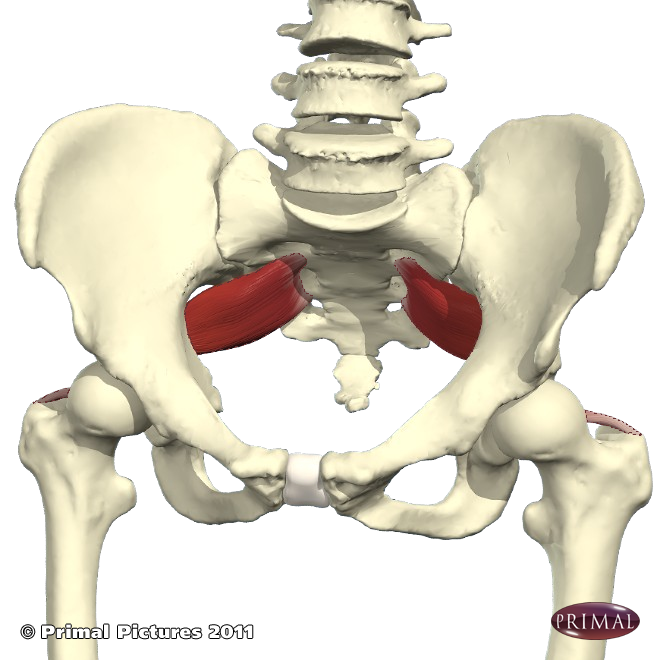
Each time I am in a gross anatomy lab, I find myself looking at the piriformis muscle and feeling a little sad. It is a muscle that is blamed for so much pain and strain in the body, yet much of the blame is sorrily misplaced and sometimes unfounded. My hope with this post is to bring a new awareness to this small muscle and what it is really trying to say.
Most yogis have a sense of where the piriformis is – and many are searching for the ultimate pose or position that will bring the ultimate piriformis stretch. Their aim is to create release and openness in the pelvis. They believe that if they release their piriformis they will overcome sciatic symptoms, piriformis syndrome, or other general and profuse “butt pain.” Basically, when “butt pain” is a topic of conversation, the piriformis muscle is right there with it. And it is anything but good.
Hence my sadness. . . .
I want everyone to know that the piriformis is a victim of the neighbourhood it resides in. Its position (deep within the pelvis) and its size (very small) lends it to being compressed and unable to “breathe” (so to speak). If it had a voice, it would say to the other hip muscles, “Would ya start working, already???” It’s doing its best to control the movement of the femur in the acetabulum, playing its part in enabling a smooth flow of energy from the upper body to the lower body and back up to the upper body. But – and it’s a big but, pun intended – it can only do so much when the other muscles are not firing or simply not working together.
Yes, it is a sad sad soap opera. The rest of the body isn’t working as well as it should, the pain arrives in the butt, and voila, we have the supposed culprit. Add to this its proximity to the sciatic nerve, and the whole blame game intensifies.
The piriformis is not at fault. Say it again. The piriformis is not at fault.
The rest of the body needs more functional synergy.
So now what?
Oftentimes the tendency is to chase after the symptom and try to resolve the problem by going after the pain. We like to avoid pain, and if we can just stretch the darn piriformis, isn’t that good enough?
Maybe. But most often not.
If you have issues that have been labelled as being related to the piriformis muscle, the issue is more widespread. Stretch the piriformis all you want, but long term the communication between the piriformis, hip flexors, abductors, adductors, and spinal muscles along with the breath needs to improve. When that happens, you shift your biomechanics, you shift your tendencies and habits, and the piriformis gets new life.
So what to do?
1. Most readers of this post will have the Therapeutic Yoga for the Shoulders and Hips book and online video, and/or the DVD. This is a great resource to explore the movement of your leg bones in your pelvis and the relationship between the pelvis and the spine and between the pelvis and the feet. If you want a copy for yourself, you can find it here – http://bit.ly/29ykcWM
2. Scale your yoga practice back a bit so that it becomes that much less about doing the pose and more about feeling the movement of your leg bones in the pelvis. Where do you compensate when you move into Triangle, Warrior 2, or Tree pose? Have someone with a keen eye analyze your movement. Do your best to not change your alignment – rather, have the person notice what is happening in the pelvis relative to the rib cage; in the pelvis relative to the spine, and in the femurs relative to the pelvis. Take a moment to truly feel.
3. Remember that you haven’t done anything wrong; you have a coagulation of tendencies and habits that have led to dysfunctional movement. You CAN become more functional. Let your issue be the guide to improvement.
In the end, the squawking of the piriformis is just your symptom for change. It is telling you that something – other than it – isn’t working. Remember it is doing its best despite the conditions surrounding it. The “neighbourhood” is full of poor communication, and when you can get the neighborhood of tissue working more effectively together, the piriformis will feel more at ease, and so will you.
If you want to take this a step further, we have 5 spots available for the April Therapeutic Yoga Intensive. This is a great opportunity to train your ability to see, to explore your own movement and compensatory strategies and really dig into improving your function and reducing/eliminating your pain. To register, click here.
Happy exploring,
Susi